Ulcerative Colitis.
A clinician-facing, evidence-anchored resource on ulcerative colitis — from Montreal extent and Truelove–Witts severity through medical escalation to the point where surgery enters the picture: acute severe colitis, colectomy, and staged restorative proctocolectomy with an ileal pouch.


 Terminal ileum — no ileitis (small bowel spared)
Anus — no perianal disease
Rectum — always inflamed (hallmark of UC)
Rectosigmoid junction (colon – rectum)
Left-sided colitis (E2) — distal to the splenic flexure
Splenic flexure — E2 / E3 boundary
Pancolitis (E3) — proximal to the splenic flexure
Terminal ileum — no ileitis (small bowel spared)
Anus — no perianal disease
Rectum — always inflamed (hallmark of UC)
Rectosigmoid junction (colon – rectum)
Left-sided colitis (E2) — distal to the splenic flexure
Splenic flexure — E2 / E3 boundary
Pancolitis (E3) — proximal to the splenic flexure
Grading a flare
The Truelove–Witts index remains the bedside anchor for classifying UC activity. Its “severe” category defines acute severe ulcerative colitis (ASUC) — the threshold for admission, intravenous steroids, and a surgical consult.
| Feature | Mild | Moderate | Severe (ASUC) |
|---|---|---|---|
| Clinical | |||
| Bloody stools/day | <4 | 4–6 | ≥6 |
| Blood in stool | Small | Moderate | Visible, frequent |
| Systemic | |||
| Temperature | Apyrexial | Intermediate | >37.8 °C |
| Pulse | <90 bpm | Intermediate | >90 bpm |
| Laboratory | |||
| Hemoglobin | Normal | Intermediate | ≤10.5 g/dL |
| ESR | ≤30 mm/h | Intermediate | >30 mm/h |
| CRP | Normal | Mildly raised | >30 mg/L* |
* CRP is a modern addition to the original 1955 criteria. ASUC = Truelove–Witts severe: ≥6 bloody stools/day plus at least one systemic sign (fever, tachycardia, anemia, or raised ESR/CRP). Endoscopic severity is scored separately by the Mayo endoscopic subscore or the UCEIS. Disease extent follows the Montreal system: E1 proctitis, E2 left-sided, E3 extensive (pancolitis).
Frequently Asked Questions
Quick, plain-language answers to the questions we hear most.
What is ulcerative colitis?
Ulcerative colitis (UC) is a chronic, immune-mediated inflammatory bowel disease of the colon and rectum. The inflammation is continuous — it begins in the rectum and extends proximally a variable distance — and is mucosal (superficial), not full-thickness. It follows a relapsing–remitting course of flares and remission. (Ordás, Lancet 2012)
What causes ulcerative colitis?
There is no single cause — UC is multifactorial. It develops when environmental triggers and an altered gut microbiome provoke a dysregulated mucosal immune response in a genetically susceptible person. No one gene, germ, food, or exposure explains it on its own; each contributes part of the risk. (Ordás, Lancet 2012)
Is UC inherited, and what is the hygiene hypothesis?
UC has a genetic component — a family history raises risk and more than 200 IBD susceptibility loci have been mapped — but it is not simply inherited, and most patients have no affected relative. The hygiene hypothesis proposes that reduced early-life microbial exposure in industrialized settings alters immune development and raises IBD risk, consistent with UC's rising incidence worldwide and in migrants who adopt a Western environment.
Why is UC called "non-full-thickness"?
UC inflammation is limited to the mucosa and submucosa — the inner lining — and does not penetrate the full thickness of the bowel wall. This distinguishes it from Crohn's disease, which is transmural (full-thickness). Because UC is superficial and confined to the colon and rectum, it does not typically cause the deep fissuring ulcers, fistulas, and strictures of Crohn's — and removing the colon and rectum is curative of the disease.
How common is UC, and who gets it?
UC is among the most common forms of inflammatory bowel disease, with a prevalence of several hundred per 100,000 in Western populations and a rising incidence globally. Onset peaks between roughly 15 and 35 years of age, with a smaller later peak, and it affects men and women about equally.
How is UC diagnosed and classified?
Diagnosis rests on colonoscopy with biopsies showing continuous mucosal inflammation extending up from the rectum, after infection has been excluded. UC is then classified by extent — Montreal E1 proctitis, E2 left-sided, E3 extensive (pancolitis) — and by severity using the Truelove–Witts criteria, the Mayo score, or the endoscopic UCEIS.
How is ulcerative colitis treated?
Most people with UC are managed medically. Treatment steps up from aminosalicylates (5-ASA) for mild-to-moderate disease, to corticosteroids for flares, then immunomodulators, biologics, and oral small molecules for moderate-to-severe or refractory disease — aiming for steroid-free remission and mucosal healing. (Ordás, Lancet 2012)
How many people with UC need surgery?
Only a minority. Historically the lifetime risk of colectomy was roughly 20–30%, but in the biologic era it has fallen — to about 10–15% at 10 years in modern cohorts. Surgery becomes necessary for medically-refractory disease, acute severe colitis that fails rescue therapy, dysplasia or cancer, or emergencies such as toxic megacolon, perforation, or severe bleeding.
What are the surgical options, and is UC curable by surgery?
Because UC lives in the colon and rectum, removing them is curative of the colonic disease. The main operations are the ileal pouch-anal anastomosis (J-pouch, IPAA), the ileorectal anastomosis (IRA), and total proctocolectomy with an end — or continent Kock — ileostomy, chosen through shared decision-making. See the Surgery section for details; for pouch-specific evidence and patient education see Pouchology and Pouchy. (ASCRS guideline, 2021)
Extent, Activity, and the ASUC Threshold
Two axes drive management in ulcerative colitis: how much colon is involved (extent) and how active the inflammation is (severity). Together they set the medical ceiling and flag the patients who cross into surgical territory.
🗺️Montreal extent (E1–E3)
E1 ulcerative proctitis, E2 left-sided colitis (distal to the splenic flexure), E3 extensive colitis (proximal to the splenic flexure, including pancolitis). Extent predicts colorectal-cancer risk, surveillance intervals, and the likelihood of eventual colectomy.
📊Severity indices
Truelove–Witts grades clinical activity at the bedside; the Mayo score combines stool frequency, rectal bleeding, endoscopy, and physician global assessment; the UCEIS standardizes endoscopic severity. Each anchors escalation decisions and trial endpoints.
🚨Acute severe UC (ASUC)
Defined by the Truelove–Witts severe criteria — ≥6 bloody stools/day plus a systemic sign. ASUC is a medical emergency requiring admission, intravenous corticosteroids, VTE prophylaxis, and early involvement of a colorectal surgeon.
🧭Extent-driven implications
Extensive, long-standing colitis carries the highest cumulative cancer risk and the strongest case for structured dysplasia surveillance — and, when disease is refractory, for definitive surgery rather than open-ended medical cycling.
Classification & severity — key references
Every reference below has been verified against PubMed and links directly to its record. This digest is educational and does not replace clinical judgement or society guidelines.
Extent & phenotype
The Montreal classification standardized how UC extent (E1–E3) and IBD phenotype are recorded, replacing ad-hoc descriptors and enabling comparison across cohorts and trials.
- Silverberg MS, Satsangi J, Ahmad T, et al. Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: report of a Working Party of the 2005 Montreal World Congress of Gastroenterology. Can J Gastroenterol. 2005;19 Suppl A:5A-36A. PMID 16151544
- Ordás I, Eckmann L, Talamini M, et al. Ulcerative colitis. Lancet. 2012;380(9853):1606-19. PMID 22914296
Severity indices
The Truelove–Witts criteria (1955) remain the operational definition of acute severe UC. The Mayo Clinic score — introduced in Schroeder’s 1987 mesalamine trial — and the UCEIS refined clinical and endoscopic scoring, respectively.
- Truelove SC, Witts LJ. Cortisone in ulcerative colitis; final report on a therapeutic trial. Br Med J. 1955;2(4947):1041-8. PMID 13260656
- Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N Engl J Med. 1987;317(26):1625-9. PMID 3317057
- Travis SP, Schnell D, Krzeski P, et al. Developing an instrument to assess the endoscopic severity of ulcerative colitis: the Ulcerative Colitis Endoscopic Index of Severity (UCEIS). Gut. 2012;61(4):535-42. PMID 21997563
This digest is educational and does not replace clinical judgement or society guidelines.
Escalation and the Medical–Surgical Decision Point
Medical management follows a step-up ladder from aminosalicylates to advanced therapies, with the goal of steroid-free remission and mucosal healing. The clinically decisive moment is when a patient exhausts or fails medical options — that is where the surgical conversation begins.
💊5-ASA (aminosalicylates)
First-line induction and maintenance for mild-to-moderate disease, oral and topical. Effective for proctitis and left-sided disease; combination oral-plus-rectal dosing improves response. Little role in severe disease or as maintenance after biologics.
🔥Corticosteroids
Rapidly control active flares but are not maintenance agents. Steroid dependence or refractoriness is itself an indication to escalate. Intravenous steroids are the backbone of acute severe UC management.
🧬Thiopurines
Azathioprine and 6-mercaptopurine provide steroid-sparing maintenance, often in combination with anti-TNF therapy to reduce immunogenicity. Slow onset limits their use for induction.
🎯Anti-TNF (infliximab)
The first biologic proven for UC induction and maintenance, and a standard rescue agent in acute severe disease. Therapeutic drug monitoring and dose optimization sustain response.
🧪Other advanced therapies
Vedolizumab (gut-selective anti-integrin), ustekinumab (anti-IL-12/23), and the oral small molecules tofacitinib and upadacitinib (JAK inhibitors) expand options for anti-TNF–exposed or refractory patients.
⏱️ASUC rescue therapy
Steroid non-responders by day 3 receive rescue with infliximab or ciclosporin. The two are comparable; the choice is driven by expertise and comorbidity. Failure of rescue is a hard indication for colectomy.
Medical therapy & escalation — key references
Landmark trials and guidelines behind the escalation ladder, each verified against PubMed. The label matters most at the point of surgical decision-making, where the surgical section takes over.
Guideline-based management
Contemporary guidelines integrate aminosalicylates, corticosteroids, thiopurines, and advanced therapies into a step-up algorithm keyed to disease extent and severity.
- Rubin DT, Ananthakrishnan AN, Siegel CA, et al. ACG Clinical Guideline: Ulcerative Colitis in Adults. Am J Gastroenterol. 2019;114(3):384-413. PMID 30840605
Biologics & small molecules
Registration trials established anti-TNF, anti-integrin, anti-IL-12/23, and JAK-inhibitor therapy for moderate-to-severe UC, progressively expanding options after 5-ASA and steroid failure.
- Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353(23):2462-76. PMID 16339095
- Feagan BG, Rutgeerts P, Sands BE, et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2013;369(8):699-710. PMID 23964932
- Sandborn WJ, Su C, Sands BE, et al. Tofacitinib as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2017;376(18):1723-1736. PMID 28467869
- Sands BE, Sandborn WJ, Panaccione R, et al. Ustekinumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2019;381(13):1201-1214. PMID 31553833
Acute severe UC rescue therapy
In intravenous-steroid–refractory ASUC, infliximab and ciclosporin achieve comparable rates of avoiding early colectomy; failure of rescue is a hard indication for surgery.
- Laharie D, Bourreille A, Branche J, et al. Ciclosporin versus infliximab in patients with severe ulcerative colitis refractory to intravenous steroids: a parallel, open-label randomised controlled trial. Lancet. 2012;380(9857):1909-15. PMID 23063316
- Williams JG, Alam MF, Alrubaiy L, et al. Infliximab versus ciclosporin for steroid-resistant acute severe ulcerative colitis (CONSTRUCT): a mixed methods, open-label, pragmatic randomised trial. Lancet Gastroenterol Hepatol. 2016;1(1):15-24. PMID 27595142
This digest is educational and does not replace clinical judgement or society guidelines.
Surgical Options for Ulcerative Colitis
Because UC is confined to the colon and rectum, surgery is curative of the colonic disease. Whether, when, and which operation to perform is individualized through shared decision-making — balancing cure, bowel function, continence, fertility, and cancer risk. Only a minority of patients ever need an operation; it is reserved for medically-refractory disease, acute severe colitis failing rescue, dysplasia or cancer, and emergencies (toxic megacolon, perforation, severe bleeding). An emergency almost always begins with a subtotal colectomy and end ileostomy, deferring the reconstructive choice until the patient has recovered.
Three options once the colon is removed
1 · IPAA (J-pouch)
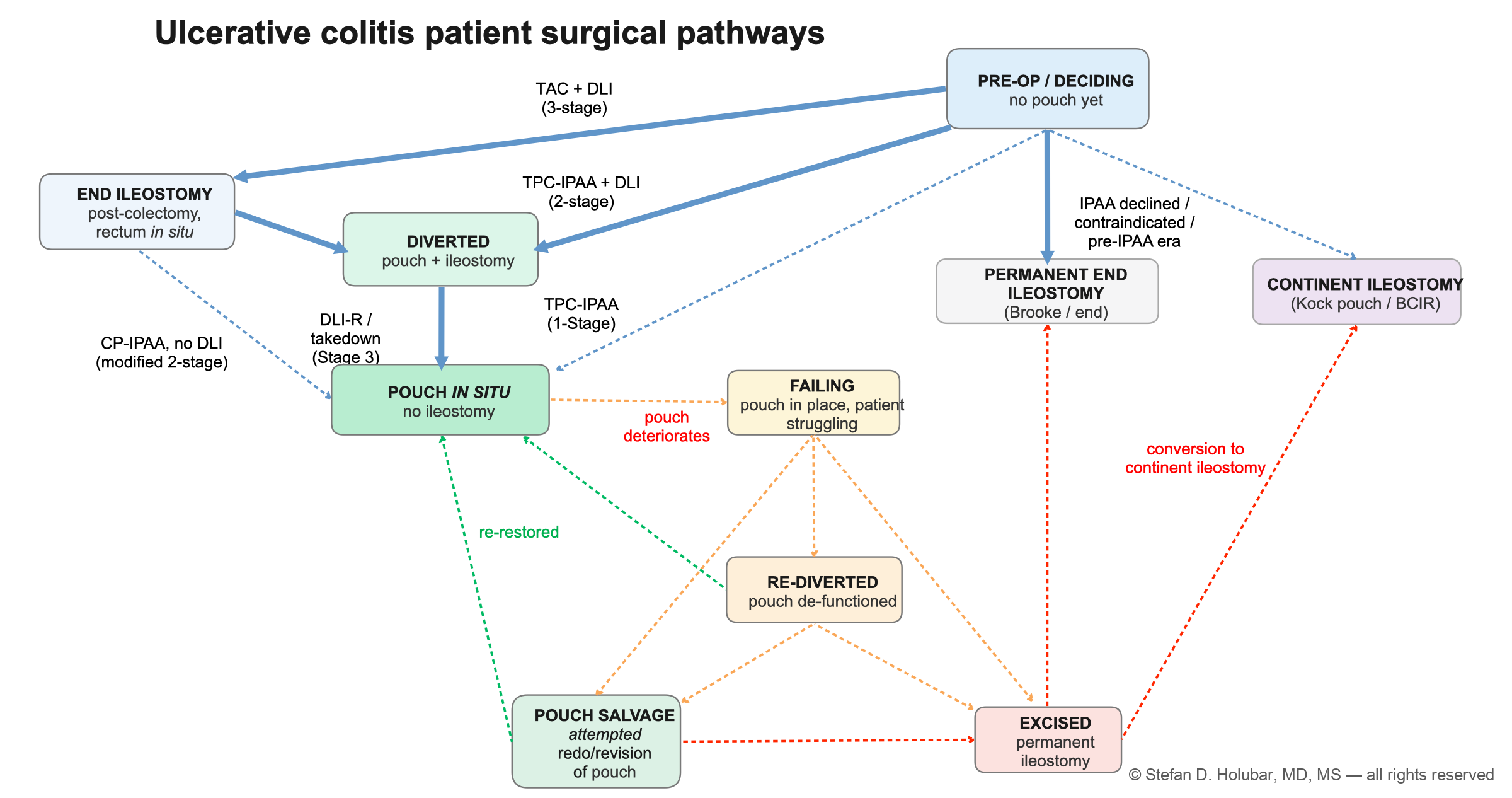
Restorative proctocolectomy with an ileal pouch-anal anastomosis: the small intestine is folded into an internal pouch joined to the anus, so stool passes normally with no permanent stoma. The standard restorative option, most often built in stages — commonly three (subtotal colectomy + end ileostomy → completion proctectomy + pouch + diverting loop ileostomy → ileostomy closure). Depends on candidacy for IPAA (below).
in progress
2 · IRA
Total abdominal colectomy with an ileorectal anastomosis: the colon is removed and the ileum is joined to a retained rectum, avoiding a pelvic dissection and a pouch. A rectal-sparing choice for selected patients (relative rectal sparing, fertility preservation, older patients, or those who decline a pouch). The retained rectum still carries disease activity and cancer risk, so it requires ongoing surveillance.
3 · TPC-EI or Kock
Total proctocolectomy with a permanent end (Brooke) ileostomy: the colon and rectum are removed with a durable, definitive stoma. Chosen for patients who are not IPAA candidates, have impaired continence, or prefer it. The continent (Kock) ileostomy is an alternative stoma-free continent option in selected patients at experienced centers.
in progress
Choosing the operation
✅Candidacy for IPAA
Candidacy for IPAA requires confirmed UC (not Crohn’s), adequate anal sphincter function and continence, and no low rectal cancer needing wide excision. Age, body habitus, comorbidity, and fertility timing all weigh in — the pouch is powerful but not right for everyone.
🤝Shared decision-making
The right operation is a shared decision between patient and surgeon, weighing cure against bowel function, continence, fertility (pelvic dissection can reduce female fertility), and the durability of each option. Patient priorities lead the conversation.
🎯Surgeon discretion & experience
Operative choice, staging, and technique also turn on surgeon discretion, training, and experience and on center volume — particularly for the pouch and the continent ileostomy, where outcomes are best in experienced hands.
📚Go deeper on the pouch
This page is an overview. For the pouch-specific evidence base see Pouchology; for plain-language, patient-facing J-pouch education see Pouchy.
Intended for healthcare professionals. Patients and families: see the plain-language version on Pouchy.
For clinicians & traineesSurgical decision-making in ulcerative colitis
A concise, evidence-anchored map of the operative decisions in ulcerative colitis (UC): when to operate, how many stages to use, which reconstruction to offer, and how to time surgery around medical therapy. Grades of recommendation below are drawn from the American Society of Colon and Rectal Surgeons (ASCRS) Clinical Practice Guidelines for the Surgical Management of Ulcerative Colitis1; every row is anchored to that guideline and to the primary evidence beneath it.
An independent educational project of Holubar Lab. The views expressed are the author's own and are not those of Cleveland Clinic or the American Society of Colon and Rectal Surgeons.
1 When to operate — indications & timing
Surgery in UC is curative of the colonic disease; the trigger is failure of medical therapy or neoplasia. Timing is individualized and, in the acute setting, benefits from early surgical involvement.
| Clinical scenario | Operation typically favored | ASCRS grade | Key considerations |
|---|---|---|---|
| Hospitalized moderate–severe UC escalating medical therapy | Early surgical consultation within a multidisciplinary team; colectomy held in reserve | 1C | About one in five UC patients is hospitalized, and roughly 20–30% of acute flares proceed to colectomy; early joint gastroenterology–surgery input typically improves timing and stoma preparation.1, 2, 3 |
| Acute severe UC (ASUC), IV-steroid-refractory at ~3–5 days | Second-line rescue therapy (infliximab or cyclosporine); colectomy if no response | 1C | Rescue therapy is typically trialed once, with colectomy for non-responders; prolonged non-operative care risks perforation and multi-system decline.1, 4, 5 |
| Fulminant colitis, toxic megacolon, or colonic perforation | Total abdominal colectomy with end ileostomy (pouch deferred) | 1C | The rectum is typically left in situ as a stump; a restorative pouch is not created in the emergent, physiologically stressed setting.1, 6 |
| Worsening ASUC in a high-risk, immunocompromised, or malnourished patient | Rescue diverting loop ileostomy may be considered to potentially avert an emergent colectomy | 2C | A selective, emerging option that can allow colonic decompression and patient optimization before more definitive surgery; not a substitute for colectomy when indicated.1, 7 |
| Colorectal cancer, or dysplasia not amenable to endoscopic excision (invisible multifocal low-grade, or any high-grade) | Total proctocolectomy, with or without IPAA | 1B | Flat low-grade dysplasia can progress to advanced neoplasia; a cancer diagnosis is managed with oncologic resection and multidisciplinary staging, and may affect pouch suitability.1, 8, 9 |
| Chronic medically refractory UC (elective) | Elective restorative or non-restorative proctocolectomy — see Tables 2–3 | 1B | The number of stages and the reconstruction are chosen together, based on nutrition, immunosuppression, sphincter function, and patient goals.1, 10 |
2 How many stages — sequencing the IPAA
For restorative proctocolectomy, a 2-stage, 3-stage, or modified 2-stage approach is preferred for most patients; the choice is individualized to acuity, nutrition, and immunosuppression.1
| Approach | What it entails | ASCRS grade | Typically chosen when |
|---|---|---|---|
| 3-stage | Total abdominal colectomy + diverting/end ileostomy → completion proctectomy with IPAA + diverting loop ileostomy → ileostomy closure | 1C–1B | Emergent or acute presentation, malnutrition, or high-dose steroids/biologics; separates the sickest phase from pelvic reconstruction to minimize anastomotic-leak and pelvic-sepsis exposure.1, 11, 12 |
| Modified 2-stage | Total abdominal colectomy + end ileostomy → completion proctectomy with IPAA without a diverting loop ileostomy | 1B | After the colon is already removed and the patient is optimized and off immunosuppression; increasingly used and, in comparative series and meta-analysis, not clearly associated with higher leak, sepsis, or pouch failure.1, 13, 14, 15 |
| Traditional 2-stage | Total proctocolectomy with IPAA + diverting loop ileostomy → ileostomy closure | 1B | Elective patient in reasonable nutritional condition and off high-dose immunosuppression; the long-standing default (about three-quarters of IPAAs are performed as 2-stage).1 |
| Single-stage | Total proctocolectomy with IPAA and no diversion | 1B | Highly selected, low-risk patients — ideal nutrition, off steroids and biologics; not appropriate for most, given the consequences of an undiverted pelvic leak.1, 15 |
A laparoscopic or robotic (minimally invasive) approach is typically preferred where expertise is available, with equivalent or improved short-term outcomes, fertility, and long-term function.1, 16, 17
3 Which reconstruction — restore continuity, or not
For elective surgery, restorative IPAA, permanent end ileostomy, and continent ileostomy are all acceptable options with quality of life approaching the healthy population; the choice is individualized to sphincter function, anatomy, surveillance needs, and patient preference.1
| Option | Typical candidate | ASCRS grade | Trade-offs to counsel |
|---|---|---|---|
| Restorative total proctocolectomy + IPAA (J-pouch) | Most patients who wish to avoid a permanent stoma and have adequate sphincter function | 1B | Quality of life approaches the healthy population; pouchitis is common; counsel on possible effects on fertility, pregnancy, sexual, and urinary function — a minimally invasive approach reduces infertility risk.1, 10, 18, 19 |
| Total proctocolectomy + permanent end (Brooke) ileostomy | Impaired sphincter/incontinence, limited physiologic reserve, surveillance barriers, or patient preference | 1B | A safe, effective, curative operation with quality of life equivalent to IPAA; a deliberate, valid choice — not a “failure” option.1, 20, 21 |
| Total abdominal colectomy + ileorectal anastomosis (IRA) | Selected patients with relative rectal sparing and a compliant, healthy rectum | 2B | Avoids a pelvic dissection (may preserve fertility) but leaves the rectum — requiring lifelong surveillance for its ongoing cancer risk; a substantial proportion eventually need completion proctectomy.1, 22, 23 |
| Continent ileostomy (Kock pouch / BCIR) | Highly selected patients in whom IPAA is contraindicated or has failed and who decline a conventional end ileostomy | 1B | Offers stoma-appliance-free continence, but carries high rates of dysfunction and reoperation/revision; performed at a limited number of centers.1, 24, 25 |
4 Timing around medical therapy
Preoperative immunosuppression influences the choice of how many stages to use more than whether to operate. The staging decision is individualized and at the discretion of the treating surgeon.
| Drug class | Effect on surgical risk | Typical implication |
|---|---|---|
| High-dose corticosteroids (>~20 mg prednisone/day) | Associated with increased postoperative infectious and septic complications | Favor a staged approach; wean where feasible before pelvic reconstruction.1, 26, 27 |
| Anti-TNF agents (infliximab, adalimumab) | Controversial; the largest series and meta-analyses report increased anastomotic leak and pelvic sepsis | A staged approach may mitigate the risk, particularly with coexisting risk factors.1, 28, 29, 11 |
| Vedolizumab, ustekinumab, tofacitinib | Limited and mixed data on postoperative outcomes | Individualize; staging is often favored when other risk factors coexist.1, 17 |
| Immunomodulators (azathioprine, 6-mercaptopurine, methotrexate) | Not associated with increased postoperative complications | The decision to stage is not typically driven by immunomodulator exposure.1, 30, 31 |
| Tofacitinib (JAK inhibitor) — VTE consideration | Adds thrombotic risk on top of an already-elevated surgical baseline | Consider extended postoperative venous thromboembolism prophylaxis in exposed patients.1, 32, 33 |
Grades of recommendation (ASCRS/GRADE): the first digit is strength (1 = strong, 2 = weak); the letter is evidence quality (A high, B moderate, C low). A weak recommendation means the best action may reasonably differ between patients.1
References
Every reference below was retrieved from the peer-reviewed literature and verified against PubMed; each links to its record. Author lists are abbreviated pending final formatting.
- Holubar SD, et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Surgical Management of Ulcerative Colitis. Dis Colon Rectum. 2021;64:783-804. PMID 33853087
- Levy LC, et al. The management of the hospitalized ulcerative colitis patient: the medical-surgical conundrum. Curr Opin Gastroenterol. 2020;36:265-276. PMID 32487850
- Kotze PG, et al. Acute severe ulcerative colitis: defining the precise moment for colectomy. Expert Rev Gastroenterol Hepatol. 2025;19:5-14. PMID 39753508
- Li Wai Suen CFD, et al. Factors Associated With Response to Rescue Therapy in Acute Severe Ulcerative Colitis. Inflamm Bowel Dis. 2024;30:1389-1405. PMID 37725044
- Bressler B, et al. The use of infliximab for treatment of hospitalized patients with acute severe ulcerative colitis. Can J Gastroenterol. 2008;22:937-40. PMID 19018340
- Arnell Tracey D. Surgical management of acute colitis and toxic megacolon. Clin Colon Rectal Surg. 2004;17:71-4. PMID 20011287
- Russell TA, et al. Rescue Diverting Loop Ileostomy: An Alternative to Emergent Colectomy in the Setting of Severe Acute Refractory IBD-Colitis. Dis Colon Rectum. 2018;61:214-220. PMID 29337777
- Ullman T, et al. Progression of flat low-grade dysplasia to advanced neoplasia in patients with ulcerative colitis. Gastroenterology. 2003;125:1311-9. PMID 14598247
- Sugita A, et al. Management of Pouch Neoplasia. Dis Colon Rectum. 2022;65:S129-S135. PMID 35895865
- Bohl JL, et al. Indications and Options for Surgery in Ulcerative Colitis. Surg Clin North Am. 2015;95:1211-32, vi. PMID 26596923
- Gu J, et al. Operative strategy modifies risk of pouch-related outcomes in patients with ulcerative colitis on preoperative anti-tumor necrosis factor-α therapy. Dis Colon Rectum. 2013;56:1243-52. PMID 24104999
- Hicks CW, et al. Possible overuse of 3-stage procedures for active ulcerative colitis. JAMA Surg. 2013;148:658-64. PMID 23700124
- Zittan E, et al. Modified Two-stage Ileal Pouch-Anal Anastomosis Results in Lower Rate of Anastomotic Leak Compared with Traditional Two-stage Surgery for Ulcerative Colitis. J Crohns Colitis. 2016;10:766-72. PMID 26951468
- Moojen TB, et al. Modified-two-stage versus three-stage approach in ileoanal pouch surgery for ulcerative colitis. J Crohns Colitis. 2026;20. PMID 41258995
- Khan K, et al. Is diversion free ileal pouch-anal anastomosis a safe procedure? A meta-analysis of 4973 cases. Int J Colorectal Dis. 2021;36:657-669. PMID 33398510
- Lee GC, et al. Minimally Invasive and Robotic Surgery for Ulcerative Colitis. Clin Colon Rectal Surg. 2022;35:463-468. PMID 36591398
- Lightner AL. Surgery for Inflammatory Bowel Disease in the Era of Biologics. J Gastrointest Surg. 2020;24:1430-1435. PMID 32253646
- Cornish JA, et al. The effect of restorative proctocolectomy on sexual function, urinary function, fertility, pregnancy and delivery: a systematic review. Dis Colon Rectum. 2007;50:1128-38. PMID 17588223
- Gorgun E, et al. Does laparoscopic ileal pouch-anal anastomosis reduce infertility compared with open approach?. Surgery. 2019;166:670-677. PMID 31420214
- Holubar SD, et al. Minimally invasive total proctocolectomy with Brooke ileostomy for ulcerative colitis. Inflamm Bowel Dis. 2009;15:1337-42. PMID 19266572
- Holubar SD, et al. When Patients With IBD Require an Ostomy: Evidence-Based Answers to 10 Common Clinical Questions in IBD Surgery. Am J Gastroenterol. 2025;120:268-271. PMID 39887123
- Scoglio D, et al. Surgical treatment of ulcerative colitis: ileorectal vs ileal pouch-anal anastomosis. World J Gastroenterol. 2014;20:13211-8. PMID 25309058
- Savitch Samantha L, et al. The Fate of the Rectum in Inflammatory Bowel Disease. Surg Clin North Am. 2025;105:423-433. PMID 40015825
- Deputy M, et al. Long-term outcome and quality of life after continent ileostomy for ulcerative colitis: A systematic review. Colorectal Dis. 2021;23:2286-2299. PMID 34166559
- Wu XR, et al. Continent Ileostomy as an Alternative to End Ileostomy. Gastroenterol Res Pract. 2020;2020:9740980. PMID 32382274
- Li J, et al. Preoperative Corticosteroid Usage and Hypoalbuminemia Increase Occurrence of Short-term Postoperative Complications in Chinese Patients with Ulcerative Colitis. Chin Med J (Engl). 2016;129:435-41. PMID 26879017
- Ritter KA, et al. Postoperative Steroid Taper Is Associated With Pelvic Sepsis After Ileal Pouch-anal Anastomosis. Inflamm Bowel Dis. 2019;25:1383-1389. PMID 30597024
- Billioud V, et al. Preoperative use of anti-TNF therapy and postoperative complications in inflammatory bowel diseases: a meta-analysis. J Crohns Colitis. 2013;7:853-67. PMID 23523418
- Sahami S, et al. A Multicentre Evaluation of Risk Factors for Anastomotic Leakage After Restorative Proctocolectomy with Ileal Pouch-Anal Anastomosis for Inflammatory Bowel Disease. J Crohns Colitis. 2016;10:773-8. PMID 26417046
- Zmora O, et al. Should ileoanal pouch surgery be staged for patients with mucosal ulcerative colitis on immunosuppressives?. Int J Colorectal Dis. 2007;22:289-92. PMID 16932926
- Gainsbury ML, et al. Preoperative infliximab is not associated with an increased risk of short-term postoperative complications after restorative proctocolectomy and ileal pouch-anal anastomosis. J Gastrointest Surg. 2011;15:397-403. PMID 21246415
- Russell TA, et al. Tofacitinib Is Associated With Increased Risk of Postoperative Venous Thromboembolism in Patients With Ulcerative Colitis. Dis Colon Rectum. 2024;67:693-699. PMID 38231035
- Larson C, et al. Postoperative Outcomes in Tofacitinib-Treated Patients With Acute Severe Ulcerative Colitis Undergoing Colectomy. Clin Gastroenterol Hepatol. 2025;23:2263-2271.e6. PMID 40239733
Surgery, IPAA & surveillance — key references
The surgical evidence base — society guidelines, pouch-outcome series, and dysplasia-surveillance consensus — each reference verified against PubMed. For the Crohn’s surgical hub see Crohnsology.org.
Guidelines & indications
Society guidelines codify the indications for colectomy, the choice of staged restorative versus non-restorative surgery, and the sequencing of operations in acute and elective settings.
- Holubar SD, Lightner AL, Poylin V, et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Surgical Management of Ulcerative Colitis. Dis Colon Rectum. 2021;64(7):783-804. PMID 33853087
- Øresland T, Bemelman WA, Sampietro GM, et al. European evidence based consensus on surgery for ulcerative colitis. J Crohns Colitis. 2015;9(1):4-25. PMID 25304060
IPAA outcomes & counseling
Large series document durable pouch survival and good quality of life after IPAA; pouchitis is the most common long-term complication, and pelvic dissection reduces female fertility — both central to informed consent.
- Fazio VW, Kiran RP, Remzi FH, et al. Ileal pouch anal anastomosis: analysis of outcome and quality of life in 3707 patients. Ann Surg. 2013;257(4):679-85. PMID 23299522
- Barnes EL, Agrawal M, Syal G, et al. AGA Clinical Practice Guideline on the Management of Pouchitis and Inflammatory Pouch Disorders. Gastroenterology. 2024;166(1):59-85. PMID 38128971
- Waljee A, Waljee J, Morris AM, et al. Threefold increased risk of infertility: a meta-analysis of infertility after ileal pouch anal anastomosis in ulcerative colitis. Gut. 2006;55(11):1575-80. PMID 16772310
Dysplasia & cancer surveillance
Cumulative colorectal-cancer risk rises with colitis duration and extent; structured surveillance with chromoendoscopy and targeted biopsy guides the decision between intensified follow-up and colectomy.
- Laine L, Kaltenbach T, Barkun A, et al. SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology. 2015;148(3):639-651.e28. PMID 25702852
- Eaden JA, Abrams KR, Mayberry JF. The risk of colorectal cancer in ulcerative colitis: a meta-analysis. Gut. 2001;48(4):526-35. PMID 11247898
This digest is educational and does not replace clinical judgement or society guidelines.
Explore the Ulcerative Colitis Surgical EvidenceLive
8,734 surgical & high-acuity ulcerative colitis studies — 6,429 (74%) with open-access full text. Search titles & abstracts, or the full text where available.
Recent abstracts
Ask AI — AI‑Powered Q&A
Ask clinical questions in plain language and get evidence‑based answers with cited sources.
About UColitis.org
UColitis.org is a clinician- and trainee-facing evidence resource for ulcerative colitis, with a deliberate surgical emphasis — classification and severity, medical escalation, acute severe UC, colectomy indications, and staged restorative proctocolectomy with an ileal pouch. It offers concise, evidence-anchored digests (every reference verified against PubMed), with an AI-powered evidence explorer and living leaderboards of the UC literature coming soon. It is the surgical companion in the IBDology family of sites: for Crohn’s surgical decision-making see Crohnsology.org, for IBD with primary sclerosing cholangitis see IBD-PSC.org, for colitis that defies the UC/Crohn’s label see IBDunclassified.org, and for the family overview see IBDology.org.

This site was created by Stefan D. Holubar, MD, MS, FACS, FASCRS, Professor of Surgery at Cleveland Clinic and the Cleveland Clinic Lerner College of Medicine & Case Western Reserve University. A fellowship-trained colorectal surgeon who specializes in inflammatory bowel disease—and, living with IBD and a J-pouch himself, a patient too—he brings both perspectives to this work. He is co-PI of the Crohn's & Colitis Foundation IBD-SIRCQ and the ACS-NSQIP IBD Collaborative, founder of the iPouch Consortium, and has authored over 300 peer-reviewed publications.
Dr. Holubar is an employee of Cleveland Clinic, and has the following disclosures: research funding from the American Society of Colon & Rectal Surgeons and the Crohn's & Colitis Foundation, and has no other disclosures or conflicts of interest.